
From PCOS to PMOS: A New Name That Reflects a Whole-Body Approach to Women's Health
Why the Name Change Matters and Why Insulin Resistance Can No Longer Be Ignored
For years, millions of women have carried a diagnosis that never quite fit.
The term Polycystic Ovary Syndrome (PCOS) has long suggested that the condition is primarily about ovarian cysts. In reality, many women diagnosed with PCOS never develop ovarian cysts at all. Instead, they experience a constellation of symptoms that affect nearly every system of the body; from metabolism and hormones to fertility, skin health, mood, and cardiovascular risk.
The recent transition to Polyendocrine Metabolic Ovarian Syndrome (PMOS) reflects a growing recognition that this is not simply an ovarian disorder. It is a complex endocrine and metabolic syndrome that deserves a more comprehensive approach to diagnosis and treatment. PMOS is now recognized as being driven by interconnected endocrine and metabolic abnormalities:
Polyendocrine: Reflects disruptions across the hypothalamic-pituitary-ovarian axis, adrenal steroidogenesis, and gonadotropin signaling; not just the ovaries. Hyperandrogenism (from both ovarian and adrenal sources) is a central feature.
Metabolic: Insulin resistance affects approximately 85% of patients and is a key driver of hyperandrogenism, dyslipidemia, type 2 diabetes risk, cardiovascular disease, and hepatic steatosis. This metabolic dimension was systematically underrecognized under the old name.
Ovarian: Ovulatory dysfunction remains a core diagnostic criterion, but the new name appropriately positions it as one component rather than the defining feature.
Why the Name Change Matters
Words shape the way we think about disease. When patients hear "polycystic ovary syndrome," many assume the problem lies solely within the ovaries. Some are even told that if they are not trying to become pregnant, there is little reason for concern. Nothing could be further from the truth.
The updated terminology emphasizes that PMOS involves multiple hormonal systems and metabolic pathways. It acknowledges that women with this condition may be at increased risk for insulin resistance, prediabetes, type 2 diabetes, dyslipidemia, nonalcoholic fatty liver disease, hypertension, and cardiovascular disease, in addition to reproductive concerns. By moving beyond the misleading "cyst" label, the new name encourages clinicians and patients alike to look deeper.
Insulin Resistance: The Hidden Driver
One of the most overlooked contributors to PMOS is insulin resistance. Insulin does much more than regulate blood sugar. It also influences ovarian function, androgen production, inflammation, and fat storage. When insulin levels remain chronically elevated, they can:
Increase ovarian androgen production
Reduce sex hormone-binding globulin (SHBG), increasing free testosterone
Promote weight gain, particularly around the abdomen
Worsen acne and excess hair growth
Disrupt ovulation and menstrual regularity
Amplify systemic inflammation
For many women, insulin resistance exists years before blood glucose or hemoglobin A1c become abnormal, making early recognition especially important.
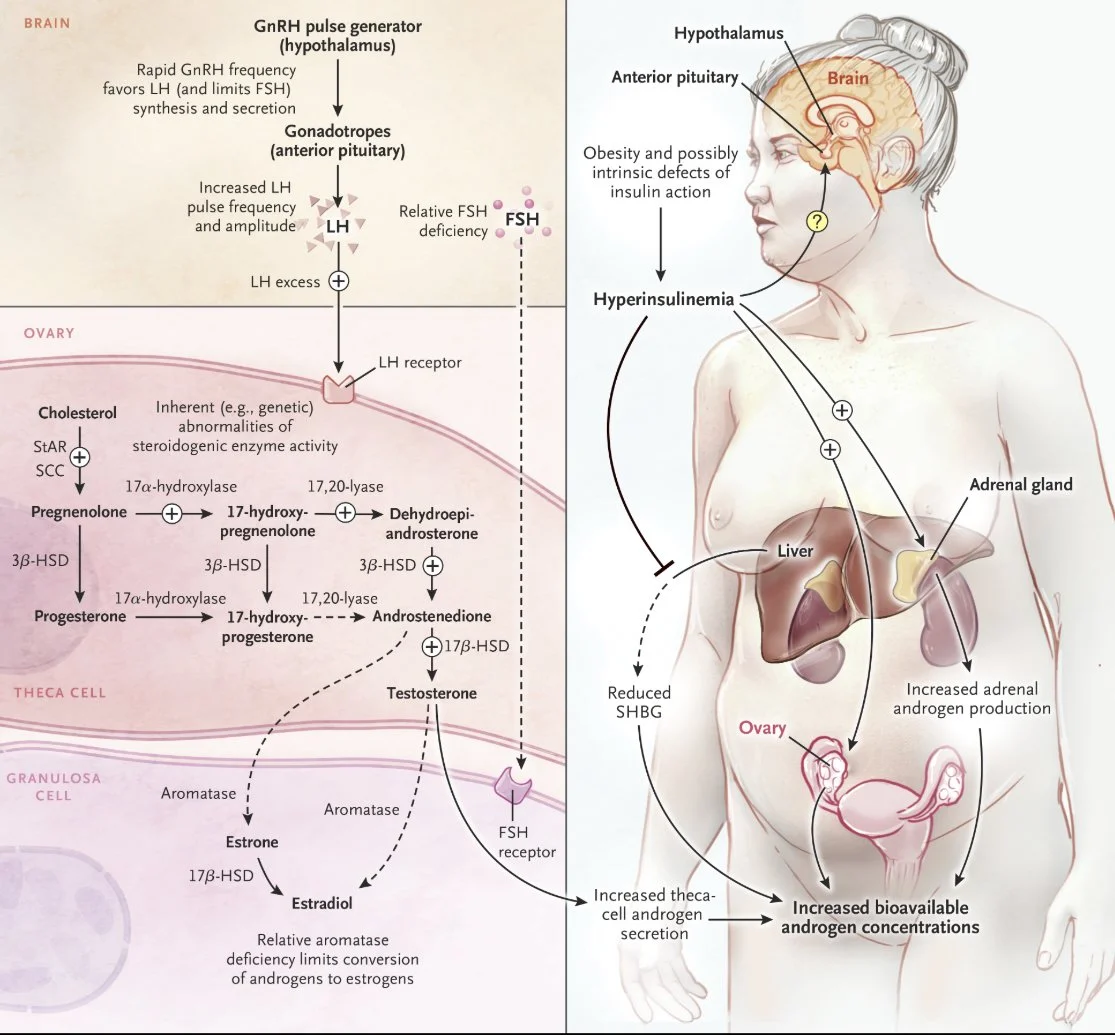
Figure 1. Basic Pathophysiology of Hyperandrogenemia in the Polycystic Ovary Syndrome.
Polycystic Ovary Syndrome. N Engl J Med. July 6, 2016.
Used under license from The New England Journal of Medicine.
My Perspective as a Practitioner
Over the years, I have cared for many women who arrived frustrated after being told that birth control pills were the primary or only treatment option for their symptoms. While hormonal contraceptives can be an appropriate and effective therapy in some patients avoiding pregnancy, they do not address the metabolic contributors that drive the PMOS. Period.
For patients with evidence of significant metabolic dysfunction, marked insulin resistance, or suspected endocrine abnormalities beyond the scope of my practice, I have often referred them to endocrinology rather than simply redirecting them back to gynecology. In my experience, collaboration with endocrinologists can be invaluable when evaluating complex metabolic and hormonal issues or considering therapies that target insulin resistance and related endocrine conditions.
At the same time, I have found that some of the most meaningful improvements occur when conventional medical care is paired with a comprehensive lifestyle strategy. This includes individualized nutrition, movement, stress reduction, sleep optimization, and evidence-informed complementary therapies like acupuncture, that support the body's capacity to heal.
The 2023 international evidence-based guidelines (which preceded and informed the name change) already recommended a paradigm shift toward recognizing PMOS as a lifelong, multisystem condition requiring integrated care:
Screening for metabolic syndrome, type 2 diabetes, cardiovascular risk factors, and sleep apnea
Routine psychological screening for depression, anxiety, eating disorders, and quality-of-life impacts
Recognition of PMOS as a higher-risk condition in pregnancy, with increased rates of gestational diabetes, preeclampsia, and birth complications
Lifestyle intervention as first-line management, with metformin recommended primarily for metabolic features
A Functional Medicine and Traditional Chinese Medicine Approach
At Tampa Bay Holistic Wellness, I view PMOS through a whole-person lens. My goal is not only to reduce symptoms but also to identify and address potential root contributors to hormonal imbalance and metabolic dysfunction. Depending on the individual, that may include:
Improving insulin sensitivity through nutrition and physical activity
Supporting healthy body composition and muscle mass
Reducing chronic inflammation
Optimizing sleep quality and circadian health
Building resilience to chronic stress
Using Traditional Chinese Medicine and acupuncture to support overall well-being and symptom management
Incorporating breathing exercises, vagal stimulation techniques, and other practices that encourage a shift from chronic sympathetic ("fight-or-flight") activation toward healthier parasympathetic ("rest-and-digest") regulation
In clinical practice, I have often observed that combining these strategies, with appropriate specialty care when necessary, can lead to improvements in energy, menstrual regularity, metabolic markers, and quality of life. Every patient is different, and treatment plans should be individualized based on goals, symptoms, and medical history.
Many of the principles I attribute as a functional medicine and Traditional Chinese Medicine doctor, like addressing root causes like insulin resistance, emphasizing lifestyle modification, using nutraceuticals like inositol, and taking a whole-systems approach, are already in fact well-supported by mainstream evidence-based guidelines for PMOS. The 2023 international guidelines for PCOS, recommend lifestyle intervention (diet and exercise) as first-line therapy, with no single regimen shown to be superior. Inositol supplementation (particularly myo-inositol in a 40:1 ratio with D-chiro-inositol) has shown efficacy for insulin resistance and ovulatory function, though metformin has greater overall efficacy in patient’s with pre-diabetes and type-2 diabetes. Other micronutrients and bacterias such as vitamin D, omega-3 fatty acids, and probiotics are often areas of deficiency in many of the client’s at risk & must be evaluated.
Looking Beyond the Ovary
The shift from PCOS to PMOS is more than a change in terminology; it represents a broader understanding of women's health.
By recognizing the endocrine and metabolic foundations of this syndrome, clinicians can move beyond treating isolated symptoms and instead focus on comprehensive, personalized care. Patients, in turn, gain a framework that validates the wide range of symptoms they may experience and highlights opportunities for prevention and long-term wellness.
For me, this name change validates what I have seen in practice for years: the most successful outcomes often come from looking beyond the ovaries and asking deeper questions about metabolism, inflammation, nutrition, stress physiology, autonomic nervous system balance, and lifestyle. When appropriate, collaborating with Endocrinology while integrating Functional Medicine, Traditional Chinese Medicine, and root-cause-oriented care has helped many patients move beyond symptom management toward lasting health improvements.
PMOS reminds us that women's health is interconnected. The ovaries do not function in isolation and neither should the way we approach their care.
References:
Polyendocrine Metabolic Ovarian Syndrome, the New Name for Polycystic Ovary Syndrome: A Multistep Global Consensus Process. Teede HJ, Khomami MB, Morman R, et al. Lancet (London, England). 2026;407(10545):2329-2339. doi:10.1016/S0140-6736(26)00717-8.
Polycystic Ovary Syndrome Perspectives From Patients and Health Professionals on Clinical Features, Current Name, and Renaming: A Longitudinal International Online Survey. Teede HJ, Moran LJ, Morman R, et al. EClinicalMedicine. 2025;84:103287. doi:10.1016/j.eclinm.2025.103287.
Polycystic Ovary Syndrome. McCartney CR, Marshall JC. The New England Journal of Medicine. 2016;375(1):54-64. doi:10.1056/NEJMcp1514916.
Polycystic Ovary Syndrome. Azziz R. Obstetrics and Gynecology. 2018;132(2):321-336. doi:10.1097/AOG.0000000000002698.
Polycystic Ovary Syndrome: Common Questions and Answers. Williams T, Moore JB, Regehr J. American Family Physician. 2023;107(3):264-272.
Recommendations From the 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Teede HJ, Tay CT, Laven JJE, et al. The Journal of Clinical Endocrinology and Metabolism. 2023;108(10):2447-2469. doi:10.1210/clinem/dgad463.
Polyendocrine Metabolic Ovarian Syndrome in Pregnancy: Pathophysiology and Outcomes. Teede HJ, Vanky E, Piltonen TT, et al. Nature Reviews. Endocrinology. 2026;:10.1038/s41574-026-01261-w. doi:10.1038/s41574-026-01261-w.
Lifestyle Changes in Women With Polycystic Ovary Syndrome. Lim SS, Hutchison SK, Van Ryswyk E, et al. The Cochrane Database of Systematic Reviews. 2019;3:CD007506. doi:10.1002/14651858.CD007506.pub4.
Nutraceuticals and Polycystic Ovary Syndrome: A Systematic Review of the Literature. Menichini D, Ughetti C, Monari F, et al. Gynecological Endocrinology : The Official Journal of the International Society of Gynecological Endocrinology. 2022;38(8):623-631. doi:10.1080/09513590.2022.2089106.
Nutritional and Herbal Interventions for Polycystic Ovary Syndrome (PCOS): A Comprehensive Review of Dietary Approaches, Macronutrient Impact, and Herbal Medicine in Management. Muhammed Saeed AA, Noreen S, Awlqadr FH, et al. Journal of Health, Population, and Nutrition. 2025;44(1):143. doi:10.1186/s41043-025-00899-y.