
Why Sex Is Plummeting And What Obesity Has to Do With It
Something unexpected is happening in modern society: people are having less sex.
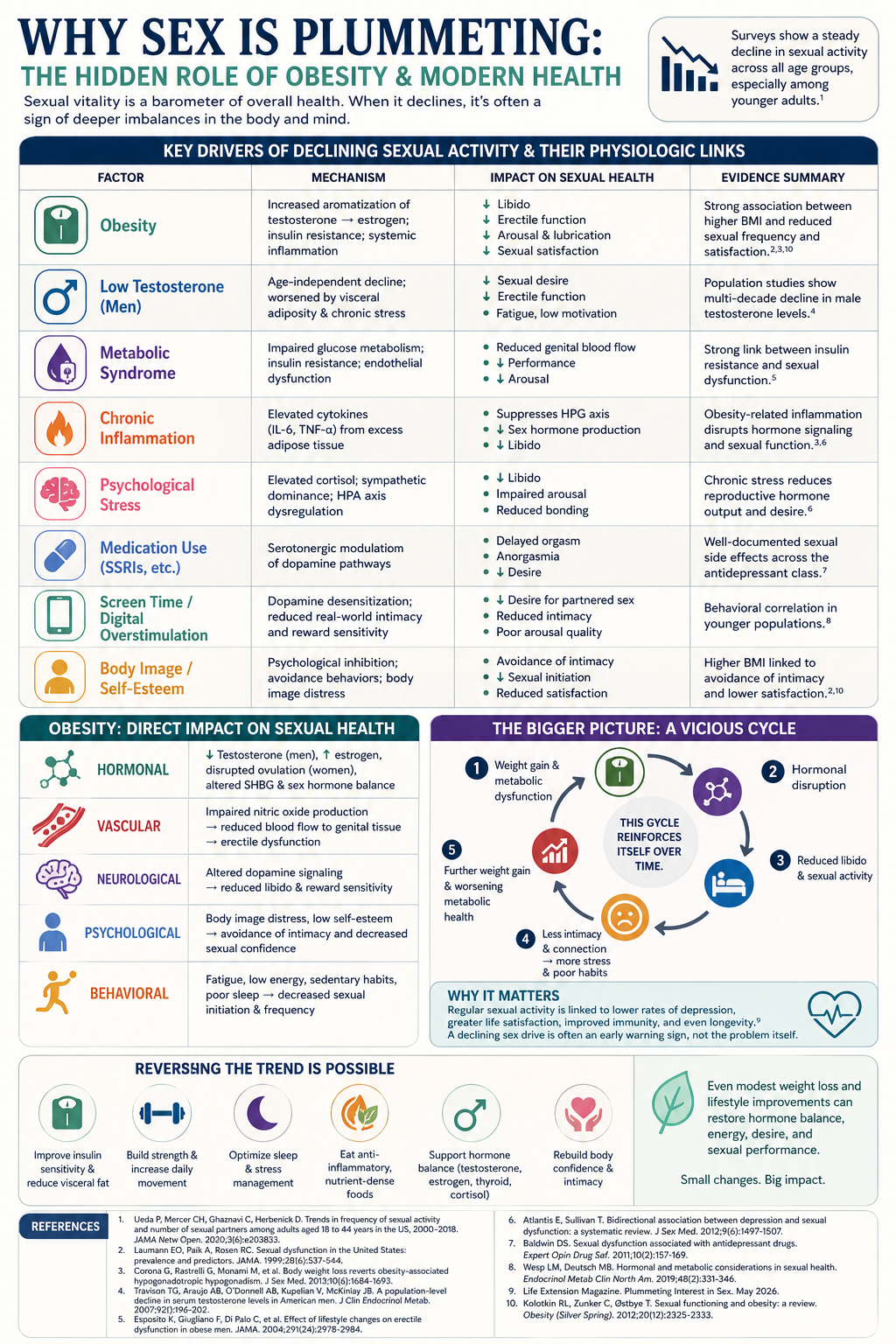
Across age groups, relationship statuses, and even cultures, sexual frequency has been steadily declining. What’s more surprising is that this trend is most pronounced in younger generations; those we typically assume are the most sexually active.
This isn’t just a cultural curiosity. It’s a health signal. Because sex, far from being just recreational, is deeply tied to hormonal balance, metabolic health, emotional wellbeing, and even longevity. So what’s driving this “sex recession”? And why is obesity emerging as one of the most overlooked contributors?
The Modern Collapse of Sexual Desire
There isn’t a single cause. Instead, we’re looking at a perfect storm of biological, psychological, and societal shifts:
Chronic stress and financial pressure
Increased screen time and digital stimulation
Social isolation and declining relationship formation
Medication side effects (especially SSRIs and other common drugs)
Declining testosterone levels in men AND women
Testosterone, in particular, plays a central role in libido, energy, and sexual function, and levels have been measurably lower in both men and women today compared to previous generations at the same age. But that’s only part of the story.
The Missing Link: Obesity and Sexual Decline
If you zoom out and look at population trends, one factor rises alongside declining sexual activity: Obesity.
Over the past few decades, rates of overweight and obesity have skyrocketed globally. At the same time, sexual frequency and desire have dropped. This is not coincidence.
1. Hormonal Disruption
Obesity fundamentally alters hormone balance:
Increased body fat raises estrogen levels
Testosterone levels decline (especially in men)
Insulin resistance disrupts endocrine signaling
In fact, nearly 45% of men with moderate to severe obesity develop a form of low testosterone known as obesity-related hypogonadism. Low testosterone = low libido, reduced sexual performance, and decreased motivation for intimacy.
2. Inflammation and Metabolic Dysfunction
Obesity is not just excess weight, it’s a chronic inflammatory state. Research shows that individuals with obesity experience:
Higher systemic inflammation
Increased metabolic dysfunction
Greater cardiovascular risk
All of these impair blood flow, energy production, and neurological signaling, key components of sexual function. For men, this often manifests as erectile dysfunction. For women, it can present as reduced arousal, lubrication issues, and hormonal imbalance.
3. Direct Impact on Sexual Desire and Frequency
Large-scale analyses consistently show:
Higher BMI is associated with lower sexual desire
Weight gain correlates with less frequent intercourse
Obesity is linked to lower sexual satisfaction across populations
This isn’t just physiological; it’s behavioral. When energy is low, inflammation is high, and hormones are dysregulated, the body deprioritizes reproduction and intimacy.
4. Psychological and Body Image Barriers
Sexual health isn’t purely biological, it’s deeply psychological.
Excess weight often contributes to:
Lower self-esteem
Body image discomfort
Avoidance of intimacy
In surveys, a significant percentage of individuals who perceive themselves as overweight report avoiding sexual situations entirely due to discomfort with their bodies. Even in stable relationships, this can quietly erode connection.
Why This Matters More Than You Think
Declining sexual activity isn’t just about relationships; it’s a marker of overall health. Research shows that individuals who engage in regular sexual activity:
Have lower rates of depression
Experience greater life satisfaction
May benefit from protective effects on mental health when sex occurs at least weekly
In other words, a declining sex drive is often an early warning sign not a standalone issue. The bigger picture: a feedback loop. Here’s where things become cyclical:
Weight gain = hormonal disruption
Hormonal disruption = reduced libido
Reduced libido = less intimacy and connection
Less connection = increased stress, depression, and poor habits
Poor habits = further weight gain
This loop reinforces itself over time.
Reversing the Trend
The good news? This is one of the most reversible patterns in modern health. Addressing root causes, not just symptoms, can dramatically improve both metabolic and sexual health:
Improving insulin sensitivity
Reducing visceral fat
Supporting testosterone and hormonal balance
Increasing movement and resistance training
Addressing inflammation through nutrition
Rebuilding body confidence and nervous system regulation
Even modest weight loss has been shown to improve hormone levels and sexual function.
Can GLP's Fix This
The answer is nuanced. GLP-1 receptor agonists appear to improve several biological components of sexual dysfunction (particularly testosterone and erectile function) in men with obesity and metabolic disease, but they do not comprehensively "fix" the full biopsychosocial picture. GLP’s alone are not the answer.
A 2026 systematic review of 10 studies (639 men) found that GLP-1RAs were consistently associated with increased total testosterone, particularly in men with obesity, type 2 diabetes, or functional hypogonadism. Importantly, unlike exogenous testosterone therapy, GLP-1RAs preserved or increased gonadotropin (LH/FSH) levels, maintaining the hypothalamic-pituitary-gonadal axis rather than suppressing it, making them a potential fertility-sparing alternative to testosterone replacement.
A randomized, double-blind, placebo-controlled crossover trial of dulaglutide in healthy, normal-weight, eugonadal men found no effect on sexual desire, HPG axis hormones, or sperm parameters after 4 weeks. This suggests GLP-1RAs do not impair libido in men without metabolic dysfunction, but also do not enhance it.
In the semaglutide vs. TRT trial, the IIEF-15 score (a validated measure of erectile function and sexual satisfaction) improved significantly only in the TRT group, not the semaglutide group, despite semaglutide's favorable effects on testosterone and sperm.
GLP-1RAs do not inherently address the behavioral patterns that contribute to obesity and its associated sexual dysfunction. While these medications reduce appetite and promote weight loss through pharmacologic mechanisms, they do not teach patients new coping strategies, modify ingrained habits, or address the psychological drivers of maladaptive behaviors.
Final Thoughts
The decline in sexual activity isn’t random, it’s reflective of deeper dysfunction in modern health. Obesity, metabolic disease, chronic stress, and hormonal imbalance are all converging to suppress one of the most fundamental human drives. And that matters. Because sexual vitality is not separate from health, it is a direct expression of it. When desire fades, it’s often the body signaling that something deeper needs attention.
References
Ueda P, Mercer CH, Ghaznavi C, Herbenick D. Trends in frequency of sexual activity and number of sexual partners among adults aged 18 to 44 years in the US, 2000–2018. JAMA Netw Open. 2020;3(6):e203833.
Travison TG, Araujo AB, O’Donnell AB, Kupelian V, McKinlay JB. A population-level decline in serum testosterone levels in American men. J Clin Endocrinol Metab. 2007;92(1):196–202.
Corona G, Rastrelli G, Monami M, et al. Body weight loss reverts obesity-associated hypogonadotropic hypogonadism. J Sex Med. 2013;10(6):1684–1693.
Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men. JAMA. 2004;291(24):2978–2984.
Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281(6):537–544.
Atlantis E, Sullivan T. Bidirectional association between depression and sexual dysfunction: a systematic review. J Sex Med. 2012;9(6):1497–1507.
Stanton AM, Handy AB, Meston CM. The effects of exercise on sexual function in women. Sex Med Rev. 2018;6(4):548–557.
Wesp LM, Deutsch MB. Hormonal and metabolic considerations in sexual health. Endocrinol Metab Clin North Am. 2019;48(2):331–346.
Life Extension Magazine. Plummeting Interest in Sex. May 2026.
Kolotkin RL, Zunker C, Østbye T. Sexual functioning and obesity: a review. Obesity (Silver Spring). 2012;20(12):2325–2333.