
The GLP-1 pathway: Understanding how it works
Endogenous glucagon like peptide-1 (GLP-1) is an incretin hormone secreted by our intestinal L-cells in response to food ingestion that regulates glucose homeostasis and appetite through multiple mechanisms. GLP-1 exerts its effects by binding to GLP-1 receptors expressed in the pancreas, brain (hypothalamus, nucleus tractus solitarius, nucleus accumbens), gastrointestinal tract, heart, liver, and kidneys. The hormone's key actions include: stimulating glucose-dependent insulin secretion from pancreatic β-cells, inhibiting glucagon secretion, slowing gastric emptying, promoting satiety through central pathways, and reducing appetite. Endogenous GLP-1 has an extremely short half-life (minutes) because it is rapidly degraded by the ubiquitous enzyme dipeptidyl peptidase-4 (DPP-4). This rapid degradation occurs even before the hormone leaves the gut, raising the possibility that some GLP-1 actions are transmitted via sensory neurons expressing GLP-1 receptors in the intestine and liver.
Why Endogenous GLP-1 "Stops Working"
A GLP-1 Pathway usually doesn’t fully “stop,” but it can become blunted or dysregulated due to modern metabolic stressors. In addition, the relationship between endogenous GLP-1 secretion and metabolic dysfunction is complex and somewhat contradictory. The evidence does not support a simple narrative that GLP-1 secretion uniformly declines with obesity or aging. However, some studies show reduced GLP-1 secretory responses to meals in obese individuals compared to lean controls, with one large study demonstrating that obese and overweight individuals had up to 20% reduced GLP-1 response to oral glucose independent of glucose tolerance status. A longitudinal study following healthy older adults over approximately 6 years found that both fasting GLP-1 and glucose-stimulated GLP-1 declined significantly with age. The key issue appears to be reduced incretin effect rather than simply reduced GLP-1 levels. In type 2 diabetes, the incretin effect (which normally accounts for >50% of meal-related insulin secretion) is diminished, meaning the pancreatic β-cells become less responsive to GLP-1 signaling even when GLP-1 is present. Thus, there appears to be a staggering correlation between metabolic syndrome, which is a constellation of several metabolic risk factors, and degraded endogenous GLP-1 signaling. People dealing with any of the below risk factors may be degrading their GLP-1 signaling:
1. Chronic hyperinsulinemia
Frequent eating + high glycemic load = constant insulin spikes
Over time = reduced incretin effect (GLP-1 signaling weakens)
2. Gut dysfunction
Low Akkermansia and Lactobacillus keystone microbiome bacteria = reduced GLP-1 secretion
Increased intestinal permeability (zonulin ↑) = inflammation which impairs GLP-1 signaling
3. Receptor desensitization
Chronic overstimulation (high glucose, frequent eating)
GLP-1 receptors in brain/pancreas become less responsive
4. Obesity-related inflammation
Cytokines interfere with hypothalamic signaling (leptin + GLP-1 resistance)
5. Dopamine dysregulation
Highly processed foods override satiety signals
GLP-1’s appetite suppression becomes less effective
Long-Term Dangers of GLP-1 Receptor Agonist Therapy
While GLP-1 receptor agonists manufacturers claim overall favorable long-term safety profiles with a 9% reduction in serious adverse events compared to controls, several specific safety concerns warrant attention. Gastrointestinal complications are the most common, with nausea (25-60%), vomiting (5-15%), and diarrhea (10-30%). More serious GI complications include gastroparesis, ileus, intestinal obstruction, and severe constipation including fecal impaction. The slowing of gastric emptying has been shown to increase the risk of pulmonary aspiration during general anesthesia or upper GI endoscopy.
Gallbladder and biliary disease represents a consistent class effect. Meta-analysis of 76 trials shows GLP-1 receptor agonists increase the relative risk of gallbladder/biliary disease by 37%, translating to 27 additional cases per 10,000 patients per year. This includes increased risks of cholelithiasis, cholecystitis, and cholecystectomy.
Thyroid concerns include a boxed warning for risk of thyroid C-cell tumors based on rodent studies and GLP-1 medications are contraindicated in patients with personal or family history of medullary thyroid cancer or multiple endocrine neoplasia type 2.
An important consideration is lean mass loss during GLP-1 therapy, which requires further study regarding long-term metabolic consequences.
Based on FDA labeling information, Below are the manufacturer-provided side effects for the 2 most common GLP-1 receptor agonists on the market
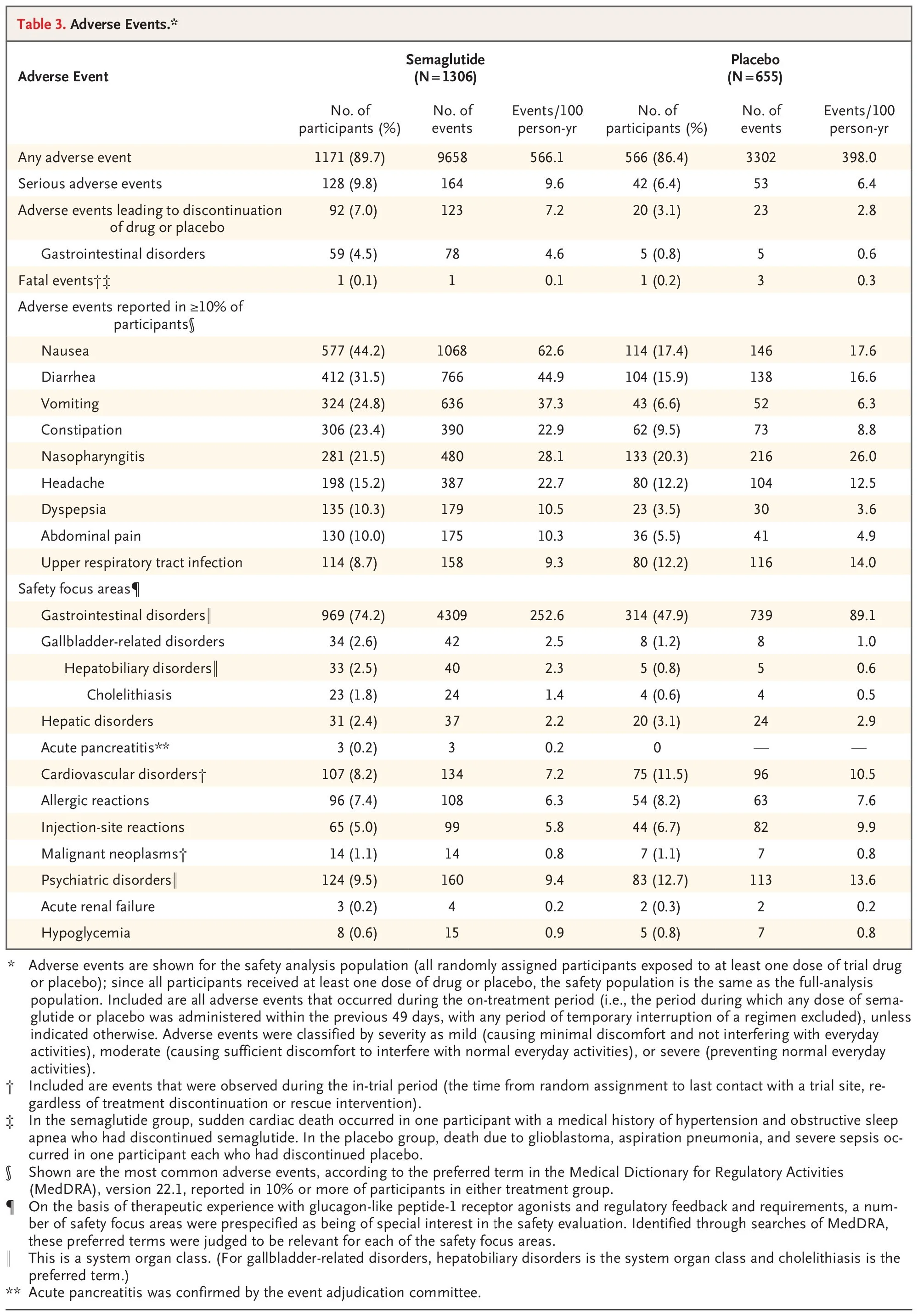
Semaglutide (Wegovy, Ozempic, Rybelsus) - Most Common Adverse Reactions (≥2% and greater than placebo):
Nausea (44%)
Diarrhea (30%)
Vomiting (24%)
Constipation (24%)
Abdominal pain (20%)
Headache (14%)
Fatigue (11%)
Dyspepsia (9%)
Dizziness (8%)
Abdominal distension (7%)
Eructation (7%)
Hypoglycemia in type 2 diabetes (6%)
Flatulence (6%)
Gastroenteritis (6%)
Gastroesophageal reflux disease (5%)
Gastritis (4%)
Hair loss (3%)
Postmarketing Adverse Reactions:
Acute pancreatitis and necrotizing pancreatitis (sometimes fatal)
Ileus, intestinal obstruction, severe constipation including fecal impaction
Anaphylaxis, angioedema, rash, urticaria
Pulmonary aspiration during general anesthesia or deep sedation
Acute kidney injury
The New England Journal of Medicine
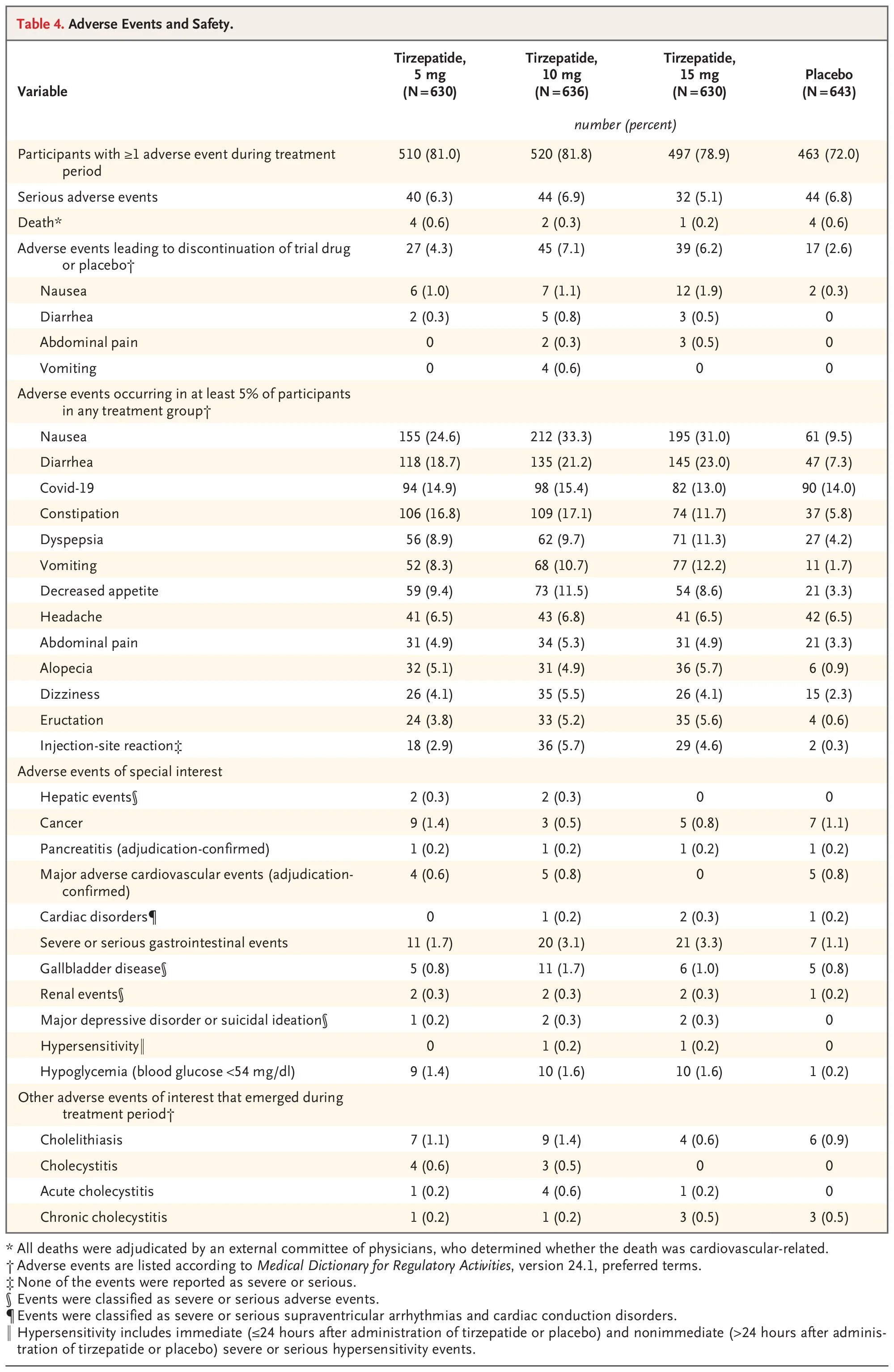
Tirzepatide (Zepbound, Mounjaro) - Most Common Adverse Events (≥5% in any treatment group):
Nausea (25-33%)
Diarrhea (19-23%)
Constipation (12-17%)
Vomiting (8-12%)
Dyspepsia (9-11%)
Decreased appetite (9-12%)
Headache (7%)
Abdominal pain (5%)
Alopecia/hair loss (5-6%)
Dizziness (4-6%)
Eructation (4-6%)
Injection-site reactions (3-6%)
Adverse Events of Special Interest:
Gallbladder disease (0.8-1.7%)
Pancreatitis (adjudication-confirmed, 0.2%)
Severe or serious gastrointestinal events (1.7-3.3%)
Hypoglycemia with blood glucose <54 mg/dL (1.4-1.6%)
The New England Journal of Medicine
Common Warnings Across All GLP-1 Receptor Agonists
All GLP-1 receptor agonists carry boxed warnings for risk of thyroid C-cell tumors based on rodent studies. Additional serious warnings include acute pancreatitis, acute gallbladder disease, hypoglycemia (when used with insulin or insulin secretagogues), heart rate increase, acute kidney injury due to volume depletion, severe gastrointestinal reactions, hypersensitivity reactions, and suicidal behavior and ideation.
This is the big-picture issue
These drugs do not fix the root cause: metabolic disease, high body fat composition regardless of BMI, insulin resistance, gut dysbiosis, and behavioral patterns. When the GLP-1 medication is stopped weight regain is common (often rapid) and appetite returns stronger than baseline. The clinical reality: GLP-1 medications are not inherently “bad” they’re just tools. GLP-1 medications make the most sense in cases of severe insulin resistance, BMI >30 (or >27 with comorbidities), and as a short-term metabolic reset (with a plan)! GLP-1 medications are problematic when used without resistance training, adequate protein, gut restoration, behavior modification, and when viewed as a permanent solution.